
Who Can Diagnose Learning Difficulties?
Dyslexia, dyscalculia, dysgraphia, specific learning disorder: what do they all mean?
A plain-language guide for families and schools.
If you have ever asked online who can assess your child for a learning difficulty, you have probably received five confident answers that all contradict each other. Some of the most common claims are simply not true. This guide sets out how it actually works in Australia. It starts with a summary and a step-by-step pathway, then goes deeper for readers who want the detail: what the DSM-5 says dyslexia means, why the word has caused so much confusion, and what good support looks like.
The short version
No law in Australia determines who can and cannot diagnose a learning difficulty. What matters is the professional’s training and competency, not their title.
Dyslexia is not a separate diagnosis. The formal DSM-5 diagnosis is specific learning disorder, and dyslexia is shorthand for one pattern of word reading difficulty within it.
A diagnosis requires difficulty that has persisted despite good teaching and targeted support. But support should start as soon as a concern is noticed. It never needs to wait for a diagnosis.
Effective intervention directly teaches the skill the child is struggling with, explicitly and step by step, and is checked with progress data. Approaches that do not directly teach reading or maths do not work.
When choosing an assessor, ask about their skills, training, and experience with learning assessments.
From concern to assessment: the pathway
If you are worried about your child’s learning, here is the practical pathway. Each step is explained more fully below.
Start with the classroom teacher. Share what you see at home and ask what the school sees. Ask what support is already in place and where your child sits compared to peers.
Ask how progress is being measured. Good support is tracked with brief, regular measures, not impressions. Ask to see the data, and ask what the plan is if progress stalls.
Give targeted support time to work, and keep records. A diagnosis requires difficulty that has persisted for at least six months despite targeted intervention, so this period is not wasted time. It is evidence. Keep copies of school reports, intervention plans, and meeting notes.
If the gap is not closing, discuss a referral. Options include the school’s wellbeing team or psychologist, a private psychologist or speech pathologist, or your GP, who can also advise on referral and rebate options. If spoken language is a concern, a speech pathology assessment may come first or run alongside.
Know what the assessment involves. A thorough assessment usually includes interviews, questionnaires for home and school, a review of the records you have kept, and individual testing across one or more sessions, followed by a written report and a feedback discussion.
Use the report as a tool. A good report informs classroom adjustments, sharpens intervention, and supports any provisions your child may be entitled to. And remember: adjustments and support at school do not require a diagnosis to begin.
There is no law about who can diagnose
This surprises many families. In Australia, there is no legislation and no government body that determines who can and cannot diagnose a learning difficulty. There are no official diagnosis regulations. What exists instead is good practice and evidence-based practice.
In practical terms, this means any professional with genuine training and competency in this area can contribute to a diagnosis. What each professional brings to the table depends on their background, training, and skills, not their job title alone.
Who does what in an assessment
A thorough learning assessment usually draws on several types of information. Different professionals are trained to gather different pieces.
Psychologists can administer cognitive assessments and academic assessments. They can also use brief language screening tools.
Speech pathologists can administer language assessments and academic assessments.
Teachers can administer academic assessments.
Speech pathologists and teachers can also use certain screening tests that are brief measures of cognitive ability.
So, there is significant overlap. However, access to a test is not the same as skill with a test. Any of these professionals can hold the testing kit. That does not mean all of them use it well, interpret it accurately, or translate the results into useful support.
There is also a practical gatekeeper – the publisher or supplier. When a professional buys an assessment tool, the publisher applies a qualification ranking system. Each test has a required qualification level, and that level dictates which professionals can purchase and administer it. This is a publisher standard rather than a law, but it does shape who uses which tools in practice.
What the psychology titles actually mean
There is a lot of misinformation about psychologists in Australia. So it’s important to clarify:
All registered psychologists are able to do assessments. However… some psychologists have skill sets that make them more confident and competent in assessing learning difficulties than others.
Legally, there are no "specialists" in Australian psychology. What the legislation provides is a system called “endorsement”. An area of practice endorsement recognises that a psychologist has completed additional accredited training in one of the following areas:
Clinical psychology
Clinical neuropsychology
Community psychology
Counselling psychology
Educational and developmental psychology
Forensic psychology
Health psychology
Organisational psychology
Sport and exercise psychology
These endorsement areas share some common skills and differ in others. They reflect additional training and a particular focus, a bit like an area of deep interest backed by formal qualifications.
Other terms you may see, such as behavioural psychologist, school psychologist, child and adolescent psychologist, or perinatal psychologist, psychotherapist are not legislated. Any registered psychologist can use those descriptions without any legal expectation of extra training behind them. That does not mean the person using them lacks skill. It means the title alone tells you nothing.
Does "generalist" mean less capable?
No. A psychologist without an endorsement is often called a generalist, or general psychologist – but generalist does not mean worse. Some generalist psychologists have more experience and competency in assessment than psychologists with an endorsement. Experience is not always better, and inexperience is not always bad. Competency is individual to each clinician.
That said, most of the time a psychologist with an educational and developmental endorsement will have the training, experience, and preference for assessing learning difficulties. This is the endorsement area most closely aligned with how children learn, how learning difficulties present, and how support can be offered in the classroom. But even here, not every educational and developmental psychologist enjoys assessment work or maintains those particular skills. The endorsement raises the likelihood of relevant expertise. It does not guarantee it.
Specific learning disorder and dyslexia: what the DSM-5 says
Here is the part that almost everyone misunderstands. Dyslexia is not a separate diagnosis in the DSM-5. There is no standalone dyslexia category with its own criteria.
The formal diagnosis is actually specific learning disorder. It is a single diagnosis that is then specified according to the academic area affected.
The diagnostic criteria, in brief
To meet criteria for specific learning disorder, all four of the following must be present:
Difficulties learning and using academic skills, shown by at least one of six symptoms lasting at least six months despite targeted intervention. The six symptoms are:
inaccurate or slow and effortful word reading;
difficulty understanding the meaning of what is read;
difficulties with spelling;
difficulties with written expression;
difficulties mastering number sense, number facts, or calculation; and
difficulties with mathematical reasoning.
The affected academic skills are substantially and measurably below what is expected for the person’s age, and they significantly interfere with academic performance, work, or daily living. This is confirmed through individually administered standardised achievement measures and comprehensive clinical assessment. For people aged 17 and older, a documented history of impairing learning difficulties can be substituted for the standardised assessment.
The difficulties began during the school-age years, even if they only became fully apparent later, when demands exceeded the person’s capacity.
The difficulties are not better explained by:
intellectual disability,
uncorrected vision or hearing problems,
other mental or neurological disorders,
psychosocial adversity,
limited proficiency in the language of instruction, or
inadequate teaching.
That is where assessment, in practice, is often more complicated than it looks. Some people have lower overall cognitive abilities but do not meet criteria for intellectual disability. Their academic skills may sit exactly where you would expect given their general thinking and reasoning skills. Is that a specific learning disorder, or simply how this person learns across the board? There is no formula that answers the question. The psychologist has to think through the results carefully, weigh the whole picture, and make the best decision they can. It is rarely simple.
The DSM-5 also adds an important note. The four criteria are to be met based on a clinical synthesis of the person’s developmental, medical, family, and educational history, school reports, and psychoeducational assessment. In other words, a diagnosis is never just a test score. It is a considered judgement drawing together information from multiple sources.
The specifiers
Once the diagnosis is made, the clinician specifies which academic domain is affected, and which skills within that domain:
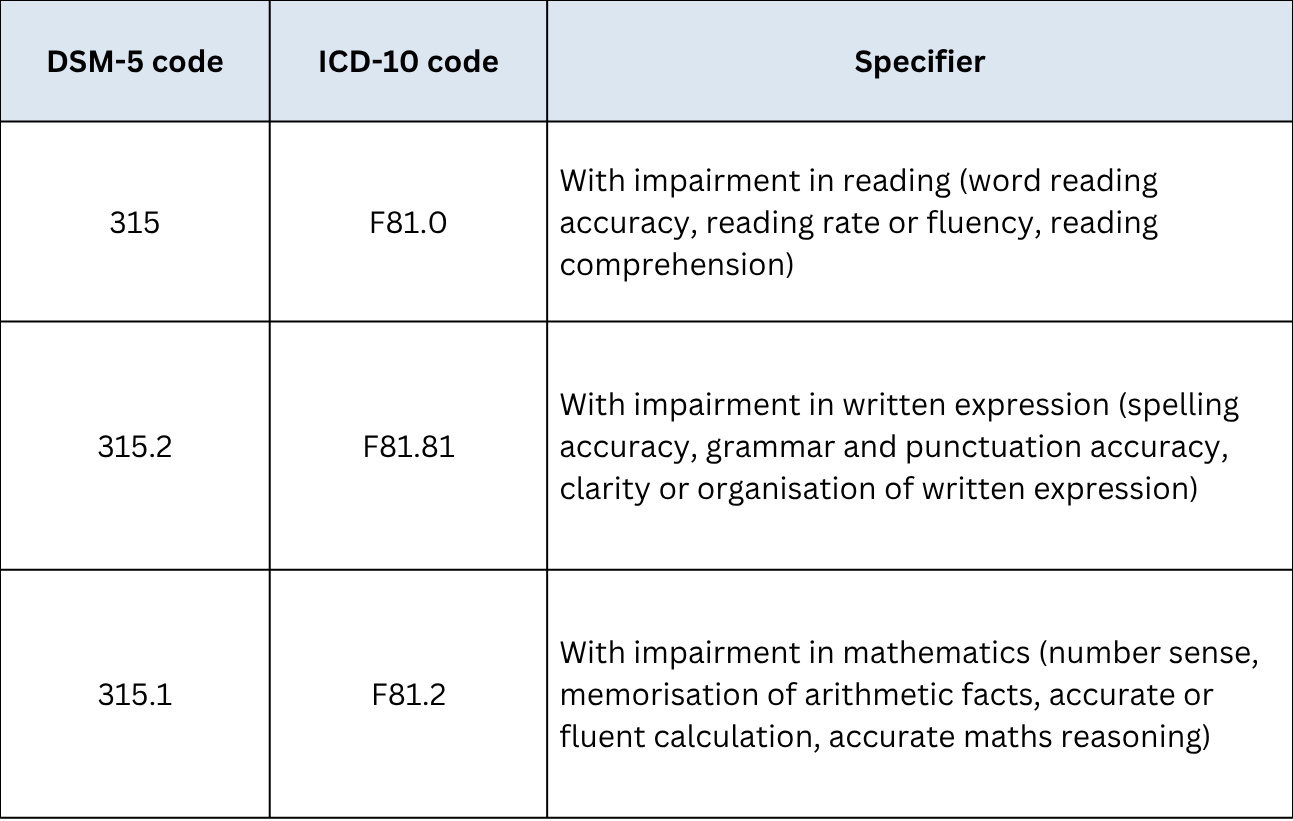
A person can meet criteria in one, two, or all three domains. When more than one domain is impaired, each is coded individually. The clinician also rates current severity as mild, moderate, or severe, based on how many domains are affected and how much specialised teaching and support the person needs to make progress. Mild difficulties may be well compensated with the right accommodations, while severe difficulties usually call for ongoing, intensive, individualised teaching across most of the school years.
So where does dyslexia fit?
The DSM-5 treats dyslexia as an alternative term, not a diagnosis. It refers to a particular pattern of difficulties within the reading domain: problems with accurate or fluent word recognition, poor decoding, and poor spelling.
So when a report says "specific learning disorder with impairment in reading", and the difficulties sit in word reading accuracy and fluency, that is the presentation most people mean when they say dyslexia. The DSM-5 notes that if the term dyslexia is used, the clinician should also specify any additional difficulties present, such as problems with reading comprehension or maths reasoning, because the word dyslexia on its own does not capture those.
The same logic applies to dyscalculia. The DSM-5 describes it as an alternative term for a pattern of difficulties within the mathematics domain: problems processing numerical information, learning arithmetic facts, and performing accurate or fluent calculations.
Dysgraphia is a little different. Unlike dyslexia and dyscalculia, the DSM-5 does not list it as an official alternative term, and in everyday use it gets applied to two quite different things. Sometimes it means difficulties with written expression, which is the specific learning disorder specifier described above. Other times it means difficulties with handwriting itself, such as letter formation, legibility, and writing speed. Handwriting difficulties are usually a motor coordination issue rather than a learning disorder, and often call for an occupational therapy assessment. So if you hear the word dysgraphia, it is worth asking which of the two is meant.
In short: specific learning disorder is the diagnosis. Dyslexia and dyscalculia are familiar shorthand for particular patterns within it. A child described as dyslexic and a child diagnosed with specific learning disorder with impairment in reading are not receiving two different diagnoses. They are receiving the same one, described two ways.
If the report says it is not dyslexia
Another thing follows from all this. If an assessment concludes that a child does not have dyslexia, or does not meet criteria for specific learning disorder, that does not mean the child has no difficulties with reading. It means the difficulties did not meet the diagnostic threshold at that point in time. Perhaps the scores were not far enough below age expectations. Perhaps another explanation fitted the picture better. Perhaps the child had not yet received enough targeted intervention for persistence to be established.
Because reading ability sits on a continuum, a child can miss a diagnostic cut-off and still be struggling in ways that are real and deserve support. The difficulties that prompted the assessment do not disappear because the label did not apply. A good report will describe what the difficulties are and recommend what should happen next, whether or not a diagnosis is made. And as this guide keeps returning to: effective support does not require the label.
Why the word dyslexia causes so much confusion
The word dyslexia has meant different things over the years, depending on the era and the theoretical background of the person using it. Each era left behind a layer of belief, and several of those beliefs are still circulating. Three are worth knowing about, because parents and teachers still run into them.
The vision myth. The term was coined in the late 1800s by eye specialists, who called the condition word blindness. That original framing never fully washed out, and it is why many people still believe dyslexia is a vision problem. Dyslexia is a language-based difficulty, sitting in how the brain maps the sounds of language onto print, not in the eyes. The DSM-5 explicitly rules out uncorrected vision problems before the diagnosis can be made.
The backwards letters myth. A 1920s theory held that children with dyslexia perceive letters and words in reverse. Later research did not support it. Reversing letters like b and d is a normal part of early reading and writing for all children, because letters are among the only objects whose identity changes when flipped. Children with reading difficulties do not see print differently from anyone else.
The bright child idea. For much of the twentieth century, dyslexia was treated as unexpected reading failure in an intelligent child. This produced the old IQ-discrepancy approach to diagnosis, discussed below. It also produced an uncomfortable pattern that Professor Julian Elliott argues continues today: which children receive the label often reflects family resources as much as anything about the child. Children with the label may access services, funding, and accommodations, while equally struggling readers without it risk being written off as lazy or slow. Same difficulty, very different treatment.
The modern understanding is clearer. Word-level reading difficulty is primarily a difficulty with phonological processing: perceiving and manipulating the sounds within words and mapping them onto letters. That is why effective intervention centres on explicit, systematic teaching of phonemic awareness and phonics. Researchers also now understand that reading ability sits on a continuum. There is no biological line where typical reading ends and dyslexia begins, so any diagnostic cut-off is a professional judgement made against agreed criteria. The difficulties are no less real for that. But the label describes the low end of a continuum, not a wholly separate category of child.
Beyond the myths, the word itself has caused practical trouble. Professor Pamela Snow (2014, 2015), a cognitive psychologist at La Trobe University, points out that in Australia dyslexia never acquired a robust, clearly fenced meaning with tight and transparent diagnostic criteria. It has been applied sometimes, by some professionals, to some children. So a parent might use it to mean any reading struggle, a teacher to mean a formally assessed difficulty, and a psychologist to mean the specific word-level pattern in the DSM-5, with each using the same word for different things. The word sounds precise and medical, and the gap between how definite it sounds and how loosely it is used is where much of the confusion lives, with families caught in the middle.
That looseness has also attracted an industry of unproven treatments. Because the word has meant so many things, programs with no evidence behind them have found it easy to claim to treat dyslexia, and families have spent large amounts of money on coloured lenses, eye exercises, movement programs, and brain training that do not work. Snow (2014, 2015) and Elliott (2014) both stress the point that matters most for families: the evidence-based interventions that help struggling readers are the same regardless of the label applied. No child needs the word dyslexia before effective reading instruction can begin.
Snow raises one further caution. A diagnostic label can let adults off the hook. If the child is seen as the problem, the quality of the instruction they received stops being examined, and a child who was never taught to read with effective methods can look identical on paper to a child with a genuine learning disorder.
None of this means reading difficulties are not real or serious. Snow and Elliott are both emphatic that they are, and that their consequences reach through a person’s academic life, mental health, and adulthood. The debate is about whether the label helps, not whether the children exist.
How diagnosis has changed
The way learning disorders were diagnosed years ago is different to now, and this adds another layer of confusion for parents comparing an older sibling’s assessment, or their own childhood experience, with a current report.
For decades, diagnosis rested on the discrepancy model that grew out of the bright child idea described earlier. A child needed a significant gap between their IQ and their reading achievement. A bright child reading poorly could be diagnosed. A child with a lower IQ reading equally poorly often could not. This approach has been largely abandoned. Children across the full range of intellectual ability can have word reading difficulties, and IQ does not predict who will respond to good reading instruction. The DSM-5 does not require any discrepancy between IQ and achievement.
What the DSM-5 asks instead is whether the academic skills are substantially below age expectations, whether the difficulties have persisted despite targeted intervention, and whether other explanations have been ruled out. That middle requirement is where response to intervention comes in.
Where response to intervention fits
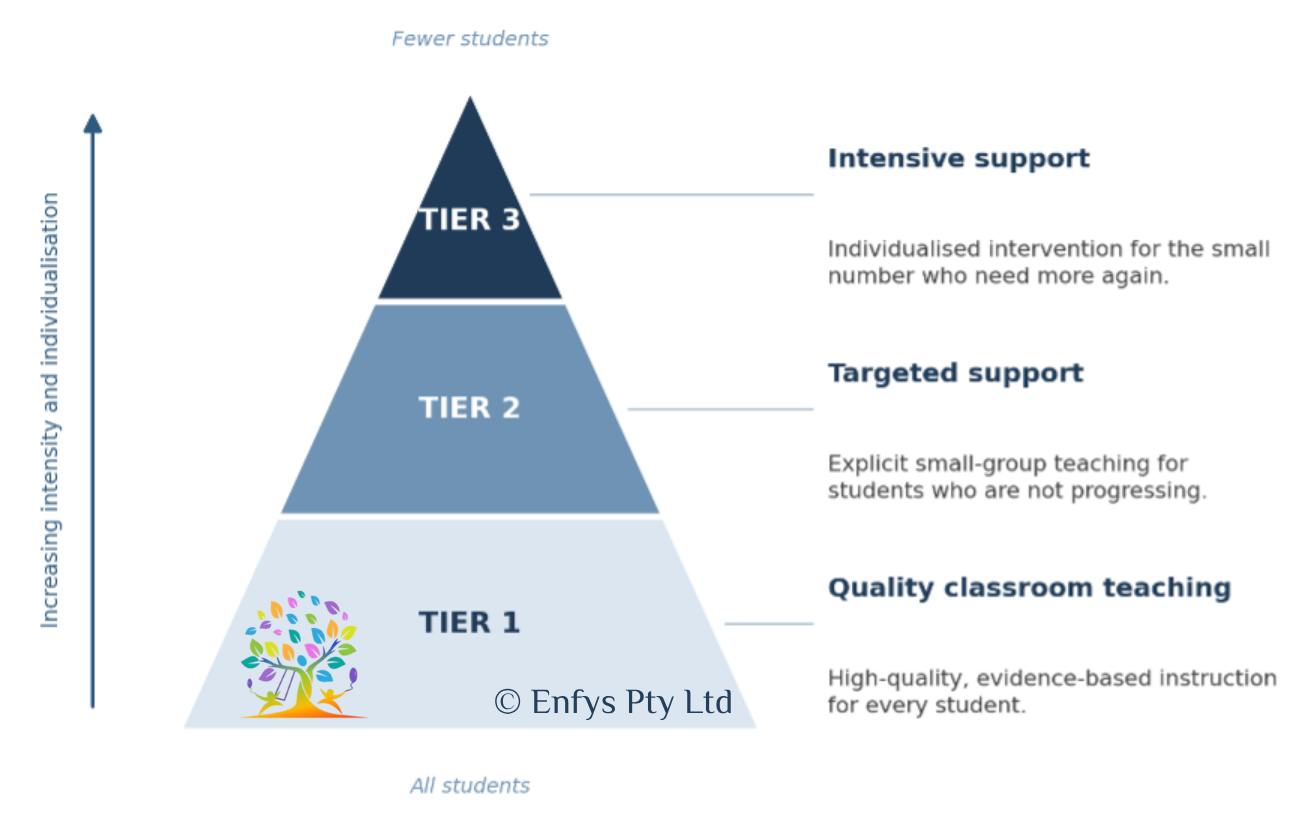
Response to intervention, often shortened to RTI, is a tiered approach to teaching and support. Tier 1 is high-quality, evidence-based classroom instruction for everyone. Tier 2 adds targeted small-group support for children who are not progressing. Tier 3 provides intensive, individualised intervention for the small number who need more again. Progress is monitored with data at every tier.
RTI matters for diagnosis because it is a key part of the DSM-5’s first criteria. The difficulties must have persisted for at least six months despite interventions that target them. A diagnosis is not meant to be made the first time a child falls behind. The question is whether the child has received good instruction and targeted support, and still not made expected progress. This is why a thorough assessment always asks about the teaching and intervention a child has already received, not just how they score on the day.
What counts as targeted intervention
The phrase "targeted intervention" is key, so it is helpful to unpack. It does not mean any extra help. It means:
extra, evidence-based instruction
matched to the student’s specific area of weakness,
delivered with increasing intensity when needed, and
checked against progress data rather than guesswork.
Each part matters.
It is extra. The child receives instruction beyond what the whole class gets. Targeted intervention is aimed at students already identified as struggling or at risk, and it works alongside classroom teaching, not instead of it.
It is matched to the specific skill. A child struggling with word reading needs intervention in word reading. This sounds obvious, but the research is clear that general cognitive training, such as working memory programs, does not improve reading or maths. Skills improve when the skill itself is taught directly.
It is explicit. The adult models the skill, guides practice, builds in cumulative review, gives immediate feedback, and works to mastery before moving on. Children with learning difficulties do not reliably pick skills up by exposure. They need them taught, step by step.
It is checked with data. Progress is measured with brief, repeated assessments, not impressions. The data shows whether the gap to peers is actually closing, and it drives the decision to continue, adjust, or intensify.
It intensifies when needed. If small-group support at Tier 2 is not producing progress, the response is to increase intensity, smaller groups or one to one, more frequent sessions, more individualisation, rather than to repeat the same dose and hope.
What professionals look for
When teachers, speech pathologists, and psychologists consider whether a child’s difficulty might be a specific learning disorder, they are each watching for slightly different things, which is exactly why collaboration works.
Teachers watch how the child responds in the classroom: the specific errors they make, whether skills stick between sessions, and whether the child is catching up to peers or the gap is widening. Speech pathologists listen for the language layer underneath: difficulties with listening comprehension, spoken language, word finding, and written language that may need their own assessment and intervention. Psychologists look for patterns across cognitive, academic, emotional, and behavioural information, and pull the whole picture together.
One point deserves emphasis. A child’s response to intervention, on its own, is not enough to identify a specific learning disorder, and neither is a single test score. Sound identification draws together academic performance, the underlying cognitive and language processes, emotional and behavioural factors, and the history of instruction. That is the clinical synthesis the DSM-5 requires.
Snow (2014, 2015) adds a caution. RTI is only as good as the quality of the classroom teaching at Tier 1. When Tier 1 instruction is strong, only a small percentage of children should need the higher tiers. Where it is weak, many children will look like they have learning difficulties when what they actually have is an instruction problem.
Making sure the support is adequate
Whether intervention is adequate is not a mystery. It can be checked. Summarised below is what that looks like from each side of the school gate – these can be used as a checklist or audit for your school to make sure appropriate supports are offered.
For teachers and schools
Use validated, evidence-based programs for intervention, built on explicit and systematic instruction. If a program cannot show evidence that it improves the skill in question, be sceptical, no matter how engaging it looks.
Match the intervention to the identified skill deficit. Reading problems need reading instruction. Maths problems need maths instruction.
Monitor progress with brief, regular measures and record the results. The question is always whether the gap to peers is closing.
Act on the data. If a term of small-group support has produced little movement, change something: intensity, group size, frequency, or program. Repeating an intervention that is not working is not persistence, it is lost time.
Coordinate. Plans are stronger when teachers, speech pathologists, psychologists, and families work from the same information, because academic skills, language, and emotional needs usually travel together.
Keep records of what was provided, for how long, and with what result. If the child is later referred for assessment, this documentation is exactly what the assessing clinician needs to apply the DSM-5 criteria properly.
Ask for help when implementation is shaky. Intervention delivered without training or fidelity rarely works, and seeking coaching or team support is a strength, not an admission of failure.
For parents
Ask what specific skill the support is targeting, and what program or approach is being used. A clear answer is a good sign. A vague one is worth following up.
Ask how progress is being measured and how often. You are entitled to see the data, not just hear that things are going well.
Ask what the plan is if progress stalls. Good support has a next step already in mind.
Keep your own file: school reports, intervention plans, meeting notes, previous assessments. If your child is later assessed, this record helps the clinician establish persistence despite intervention, which is central to the diagnosis.
Be cautious about programs that do not involve directly teaching reading or maths, however sincere the people selling them.
Watch the child, not just the scores. Homework battles, avoidance of reading, and comments like "I’m dumb" are important information. Share them with the school and any assessing clinician, because emotional wellbeing is part of the picture, not a side issue.
Choosing a professional
So how do you actually pick someone? A few things to consider:
Ask about skills and training. Any competent professional will be happy to tell you about their experience with learning assessments. This question matters far more than the title on the door.
Get recommendations from families who have actually been through an assessment.
Fit matters. A professional who was wonderful for one child may not connect as well with another. Sometimes the personal and professional match just does not work, and that is okay.
A report you were not happy with is rarely wasted money. It provides a baseline and useful information for the next assessment.
Many professionals across psychology, speech pathology, and education have genuine skill in this space. The most useful question is never what type of professional someone is, but whether they have the competency for this particular work. And whatever stage you are at, remember that effective support does not wait for a diagnosis. It can start today, in the classroom, while the bigger questions are being answered.
This is the work I do. I’m Kate Crosher, a psychologist with endorsements in educational and developmental psychology and clinical psychology, and learning assessments are the core of my practice. You can find out more about me HERE.
Every assessment I do is built around your questions, not a standard battery, and I answer them directly. You get more than scores: a full picture of how you, or your child thinks, learns, and solves problems, and how that shapes their academics, grounded in the most up-to-date model of learning difficulties (the Cattell-Horn-Carroll model of cognitive abilities).
If you’re wondering whether an assessment is the right next step, get in touch HERE. I’m happy to talk it through before you commit to anything.
If you would like to share this article in your networks, please click the button below and a PDF will automatically download into your browser.
Thanks for reading and sharing - any questions, just get in touch at admin@enfyspsych.com
References and further reading
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Elliott, J. G., & Grigorenko, E. L. (2014). The dyslexia debate. Cambridge University Press.
Grigorenko, E. L., Compton, D. L., Fuchs, L. S., Wagner, R. K., Willcutt, E. G., & Fletcher, J. M. (2020). Understanding, educating, and supporting children with specific learning disabilities: 50 years of science and practice. American Psychologist, 75(1), 37–51.
Snow, P. (2014, March 1). Dyslexia, we need to talk. It’s not me, it’s you. The Snow Report. https://pamelasnow.blogspot.com/2014/02/dyselxia-we-need-to-talk-its-not-me-its.html
Snow, P. (2015, August 14). Dyslexia dystopia. The Snow Report. https://pamelasnow.blogspot.com/2015/08/dyslexia-dystopia.html